
Education & Resources
Renal Physicians
about | home
| |
|
|
Education & Resources Renal Physicians |
communication | vision about | home |
Dear Nephrolers:
Last week we had a discussion on how to cannulate an immature fistula which the staff was infiltrating upon cannulation. I related that we study these patients and usually find lesions. When these lesions are corrected the fistulae usually work well and in a very
short time.
I thought that an illustrative case with X-rays would better make the point.
A women came in this week with a 3+ month old fistula which was infiltrating with most dialysis attempts. Upon studying her we found a stenosis at the arterial anastomosis (1 in fig 1), in the fistula central to the anastomosis (2 in fig.1) and in the fistula near the elbow (arrow in fig 2). Over two sittings the fistula was angioplastied at each area mentioned (fig. 3, 4 and 5). The results are in figures 6 and 7.
This fistula had been difficult to cannulate because of a combination of limited inflow and high venous pressure within the lumen. She went directly to dialysis after the second procedure and used the fistula for the first time without difficulty. This is our approach. It has helped us a lot. Any questions? I do hope that this is understandable.
Donald Schon, MD, FACP
AKDHC Surgery and Vascular Access Center
Phoenix, Az
(To View Original Image Click on Thumbnail)
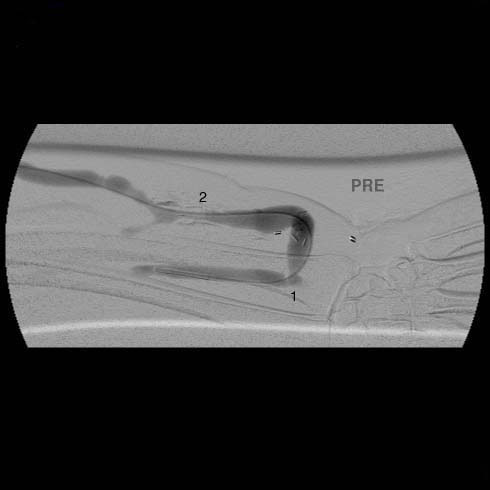
1 is the arterial anatomotic lesion and 2 is a stenosis in the
fistula |
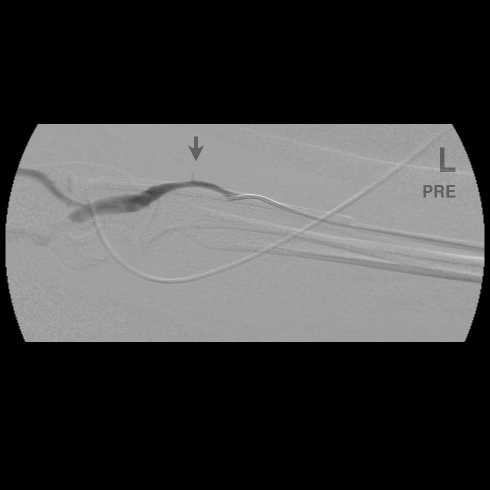
Fig 2 lesion at arrow is in the fistula just distal to the elbow.
|
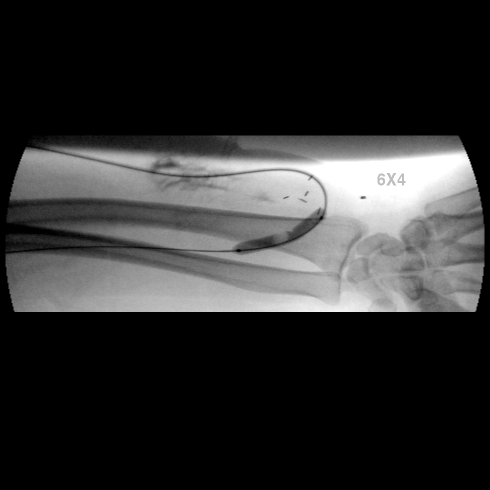
Fig 3 balloon in arterial anas
|
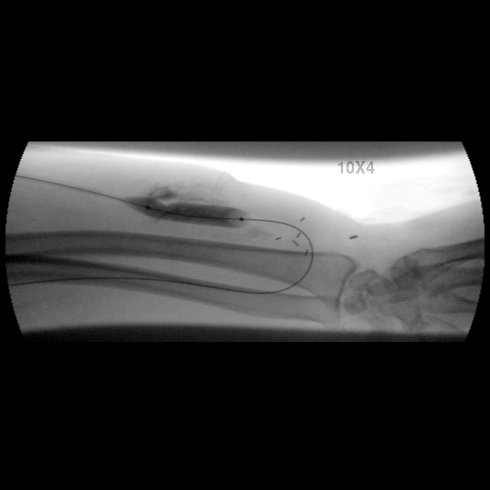
Fig 4 balloon in distal fistula lesion (2) |
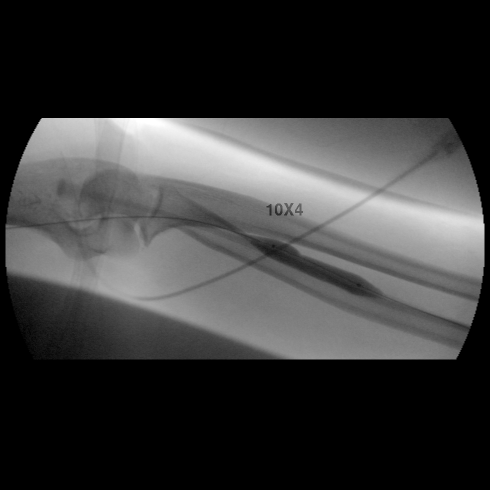
Fig 5 balloon at elbow lesion
|
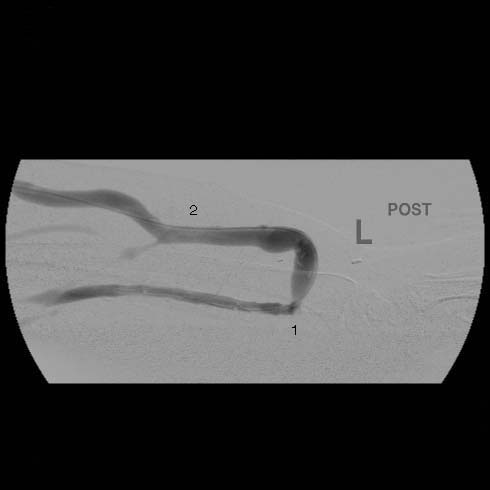
Fig. 6 post PTA of fig. 1. Note correction of stenoses at 1 and 2
|
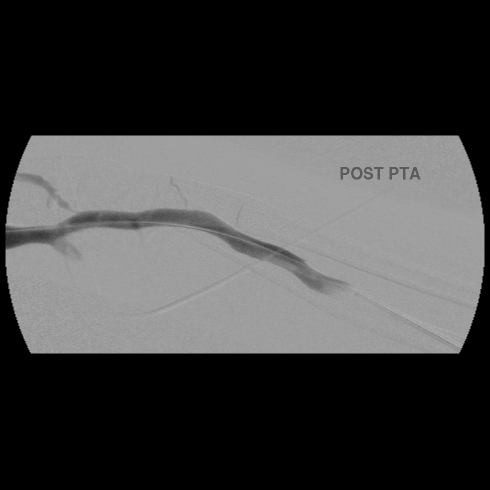
Fig 7 note correction of stenosis |
| Copyright © 2000-2007 cyberNephrologyTM
All rights reserved. Last Modified: Thursday March 08, 2007 05:21:11 PM |
info@cybernephrology.org |